The answer is simple (see below and feel free to magnify).
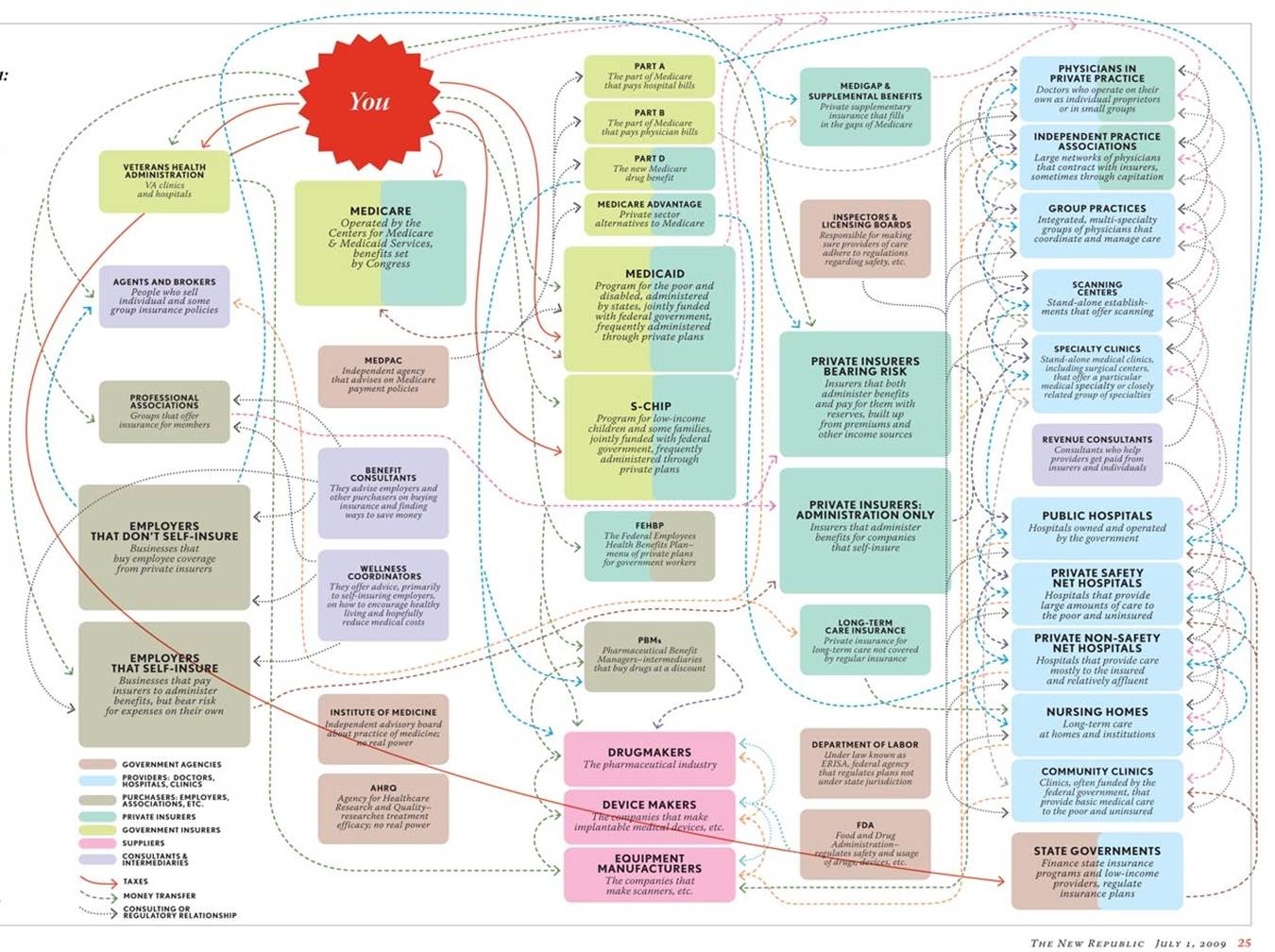
Of course, I am joking. The US health care system is a complicated web of private insurance, safety net providers, emergency rooms, etc. With so many options--or in some cases so few due to barriers--it is no wonder that people have difficulty in navigating the system!
Many underserved patients seek care from a part of the health care system known as the safety net.

The health care safety net refers to health care workers, hospitals, and clinics that offer quality health services to vulnerable populations of patients including those who are uninsured or have Medicaid. Athens is home to a few of these providers. They include the Athens Nurses Clinic, Mercy Health Center, and the Athens Neighborhood Health Center.
Just how adequate is the safety net in addressing patient needs? Let's take a look Athens Neighborhood Health Center (ANHC) and at community health centers in general.
ANHC is our local version of the national community health center (CHC). A CHC is a primary care clinic that provides services to patients regardless of their insurance status or ability to pay. In June 2012, ANHC was promoted to a Federal Qualified Health Center (FQHC). FQHC status means that the center can receive more money from the federal government in order to provide better care to more patients. In general, CHCs provide quality, primary care to patients without regard to the patient's insurance status or ability to pay. In 2010, health centers served over 20 million patients at 8,100 sites.
A few policies are in place to expand the services that CHCs can provide. The Affordable Care Act (aka Obamacare) gives CHCs $11.5 billion over the next 5 years to build new centers and to expand services provided by current ones. In addition, about one-third of CHC patients are covered under Medicaid. Under the ACA, states that choose to expand their Medicaid programs could potentially see an influx of funding to CHCs because more patients will be covered. These policies help CHCs in that they provide additional funding to support their activities; however, they do not address the lack of specialty care in such settings.

Last semester, I researched policy alternatives to increase access to specialty care (neurology, women's clinic, dental services, mental health) in CHCs. From this, I found four possible alternatives:
1. Status quo or "Tin Cup" model--This is based on charity care from local specialists. It is arranged by CHC providers through their informal networks.
2. Medicaid expansion--States that choose to expand Medicaid will, potentially, see an influx of funding to CHCs and can, therefore, use this extra money to increase specialty care provision.
3. Hiring specialists onsite--CHCs can use ACA expansion funds to hire specialists and to buy equipment for onsite use.
4. Collaboration with local public health infrastructure--CHCs can engage in contracts with local hospitals to coordinate speciality and primary care based on existing infrastructure.
After conducting a thorough literature review and evaluation, I concluded that the best-case scenario is for CHCs to collaborate with local hospitals (if available) or to hire onsite specialists (if hospitals are not available).

1. Status quo or "Tin Cup" model--This is based on charity care from local specialists. It is arranged by CHC providers through their informal networks.
2. Medicaid expansion--States that choose to expand Medicaid will, potentially, see an influx of funding to CHCs and can, therefore, use this extra money to increase specialty care provision.
3. Hiring specialists onsite--CHCs can use ACA expansion funds to hire specialists and to buy equipment for onsite use.
4. Collaboration with local public health infrastructure--CHCs can engage in contracts with local hospitals to coordinate speciality and primary care based on existing infrastructure.
After conducting a thorough literature review and evaluation, I concluded that the best-case scenario is for CHCs to collaborate with local hospitals (if available) or to hire onsite specialists (if hospitals are not available).
It is interesting, though, to be an idealistic undergraduate student. I presented this research this past Monday at the 2013 UGA CURO Symposium, and a member of the audience was a physician who had actually tried to collaborate with hospitals to arrange for specialty care in CHCs. It did not go over well. He said that at every level of hospital bureaucracy, he faced red tape and POLITICAL UNFEASIBILITY. None of the hospital administrators wanted to collaborate.
This experience has taught me two things. First, as great as it is to do policy analysis and to find the best of all possible worlds, the reality is we can not implement the best choice. It would be more realistic to work within the constraints, and, in this case, maybe the political feasibility is so insurmountable that Medicaid expansion, though shady, is actually the better alternative. (Heaven forbid it is do nothing status quo..) Second, despite all of the changes that have been made with the ACA, there are still many challenges ahead for social justice in health care.
To be continued...
This experience has taught me two things. First, as great as it is to do policy analysis and to find the best of all possible worlds, the reality is we can not implement the best choice. It would be more realistic to work within the constraints, and, in this case, maybe the political feasibility is so insurmountable that Medicaid expansion, though shady, is actually the better alternative. (Heaven forbid it is do nothing status quo..) Second, despite all of the changes that have been made with the ACA, there are still many challenges ahead for social justice in health care.
To be continued...
No comments:
Post a Comment