On Tuesday nights, I volunteer at Mercy Health Center and get to experience what it is like to seek care at a free clinic. Below is a description of the typical day and challenges that I have seen at Mercy. (Patient names and specific details will not be presented.)
Imagine yourself as a patient at Mercy Health Center. When you first walk through the clinic doors, you enter a large waiting room that seats roughly fifty people. It is packed with patients of all ages: children, adults, the elderly, and, sometimes, young adults. The atmosphere is friendly; however, you feel nervous because it is your first time at the clinic and you do not know what to expect. Or, maybe you feel self-conscious because you are going to a free clinic and hope that the people around you do not judge. You walk to the front-desk to check in and are greeted by some friendly volunteers who look a little too young to be health care professionals. They ask you to sign in on a sheet of paper and, when you finish, they put your chart up for the triage team to take you in.
When its finally your turn to see the doctors (the wait could take 10 minutes to near an hour depending on how far behind the doctors are in seeing patients), a triage nurse calls takes you back to take your vital signs (blood pressure, temperature, etc). You look around the walkway and see seven examination rooms, seven prayer rooms, booths for social services, a pharmacy, and large central stations where volunteers...
The atmosphere at Mercy is friendly; however, many patients have told us about their feeling of being stigmatized for going to a free clinic. As volunteers, we try to reduce the stigma by being professional during clinic, striking up conversations with patients, and being supportive when they need help. At MHC, I volunteer at the front desk and usually get to interact with every patient who walks through the doors. Oftentimes, I am the first friendly face that people see when they come to Mercy, and sometimes a simple "Hi, welcome to Mercy Health Center" seems to bring patients relief.
The biggest barrier to accessing care that I have seen at Mercy is a patient's ability to make it to the clinic on time. This can be challenging because patients have to work multiple jobs. However, the clinic is flexible in that it provides nighttime hours from 5-8pm Tuesday through Wednesday. Oftentimes, patients will call on the day of their appointment to say that their car broke down or they no longer have a way of getting to the clinic. Patients have even had their cars break down on site, and we have sent volunteers out to jump cars. Something that could be beneficial for Mercy patients, I think would be some sort of service to help patients get to clinic if they are unable to; however, I think this is not very feasible financially.
Given that the clinic is run completely on grant funding, volunteer help from both students and practicing health care workers, and a dedicated staff, it is amazing the variety of services that the clinic can offer. Gynecologists, optometrists, dentists, and even neurologists make monthly rounds at the clinic. In 2012 alone, Mercy saw over 10,000 patients. Though they only fill a small part of the large need within our community, Mercy is an integral part of the Athens safety net and hopefully it can continue to grow.
Friday, April 26, 2013
Monday, April 15, 2013
Mobile health technology--can it help the underserved? Part II
There are several ways that mobile technologies are used in Georgia to increase access to health care, especially in remote locations.
How are providers applying mobile health?

^ Nurses and physicians using a telemedicine cart to examine a patient.
How are universities, professors, and students involved?
In 2005, Georgia Institute of Technology and Emory University partnered to create the Health Systems Institute to research and develop new technologies that transform health care delivery. The program offers Masters and PhD tracks for students who are interested in studying such fields. HIS's research goals include managing chronic diseases, creating patient-centered technologies, robotics/medicine, and telehealth. In 2010, HIS developed a robot named Cody that can give patients bed baths:
What about patients in Athens?
 Athens Regional Medical Center (ARMC) provides a Mobile Mammography Unit, a bus that provides the staff and equipment needed to screen for breast cancer in the community. ARMC bought the bus using employee donations, and use of the bus is free. However, patients (or community sponsors such as churches) have to pay for the mammograms themselves. These services can cost up to $250 a person for those who are uninsured...
Athens Regional Medical Center (ARMC) provides a Mobile Mammography Unit, a bus that provides the staff and equipment needed to screen for breast cancer in the community. ARMC bought the bus using employee donations, and use of the bus is free. However, patients (or community sponsors such as churches) have to pay for the mammograms themselves. These services can cost up to $250 a person for those who are uninsured...
Telemedicine and mobile health is a budding field, and questions remain. What are the ethics of using such technologies, especially when it comes to using them for the underserved? By replacing a human's touch with a robot's cold arm to increase access to care, are we really fighting for a preferential option for the poor? Also, even though people are developing these technologies, how can we ensure access to those who cannot afford such services? How can the government or hospitals regulate mobile apps to make sure that they pass a benchmark quality test to be used effectively?
Stay tuned for an interview (hopefully) with the Athens Neighborhood Health Center where I will ask them more about mobile technologies...
Sources:
(1) ARMC Mobile Mammography Unit: http://www.athenshealth.org/MobileMammographyUnit
How are providers applying mobile health?
In 80% of Georgia's county health departments (ie. Clarke County Main Health Department), nurses and doctors are using video communication with the staff at the Georgia Department of Public Health. These web links are used to coordinate emergency response, train local providers, and manage epidemics.
Along with this, Georgia's Public Health Department is providing 14 telemedicine carts (computers with webcams and diagnostic equipment where physicians examine patients remotely with the help of an onsite nurse). These carts can be used in schools, prisons, nursing homes, and private offices to provide care to more people. Last year, 70,000 people were seen using a telemedicine cart. This potentially increases access to specialty care for patients located in remote areas...a possible future policy for MUAs and CHCs??
Along with this, Georgia's Public Health Department is providing 14 telemedicine carts (computers with webcams and diagnostic equipment where physicians examine patients remotely with the help of an onsite nurse). These carts can be used in schools, prisons, nursing homes, and private offices to provide care to more people. Last year, 70,000 people were seen using a telemedicine cart. This potentially increases access to specialty care for patients located in remote areas...a possible future policy for MUAs and CHCs??
^ Nurses and physicians using a telemedicine cart to examine a patient.
How are universities, professors, and students involved?
In 2005, Georgia Institute of Technology and Emory University partnered to create the Health Systems Institute to research and develop new technologies that transform health care delivery. The program offers Masters and PhD tracks for students who are interested in studying such fields. HIS's research goals include managing chronic diseases, creating patient-centered technologies, robotics/medicine, and telehealth. In 2010, HIS developed a robot named Cody that can give patients bed baths:
What about patients in Athens?
 Athens Regional Medical Center (ARMC) provides a Mobile Mammography Unit, a bus that provides the staff and equipment needed to screen for breast cancer in the community. ARMC bought the bus using employee donations, and use of the bus is free. However, patients (or community sponsors such as churches) have to pay for the mammograms themselves. These services can cost up to $250 a person for those who are uninsured...
Athens Regional Medical Center (ARMC) provides a Mobile Mammography Unit, a bus that provides the staff and equipment needed to screen for breast cancer in the community. ARMC bought the bus using employee donations, and use of the bus is free. However, patients (or community sponsors such as churches) have to pay for the mammograms themselves. These services can cost up to $250 a person for those who are uninsured...Telemedicine and mobile health is a budding field, and questions remain. What are the ethics of using such technologies, especially when it comes to using them for the underserved? By replacing a human's touch with a robot's cold arm to increase access to care, are we really fighting for a preferential option for the poor? Also, even though people are developing these technologies, how can we ensure access to those who cannot afford such services? How can the government or hospitals regulate mobile apps to make sure that they pass a benchmark quality test to be used effectively?
Stay tuned for an interview (hopefully) with the Athens Neighborhood Health Center where I will ask them more about mobile technologies...
Sources:
(1) ARMC Mobile Mammography Unit: http://www.athenshealth.org/MobileMammographyUnit
Mobile health technology--can it help the underserved? Part I
This past week, a classmate presented her project on how mobile health technology provides medical advice and reminders to people who live in remote areas that have limited access to physicians. I am curious to see how these ideas are used in the US, and specifically Athens.
First, some background.



You're probably thinking, "Sounds great. How does this work in my community??" There are several layers to how mobile technologies are applied in Athens, Georgia to improve health. Stay tuned for part II.
What is mobile health?
Mobile health technologies use mobile communication devices such as cell phones and tablet computers to provide health services.
What health services can mobile technologies provide?
Services are currently centered on preventive health and monitoring as opposed to treatment:
-reminder texts to take medications
-tracking the spread of diseases
-giving health workers a way to keep electronic records about a community's health
Cons:
-technologies are not yet tested for impact on health
-technology is not reliable: phones can run out of batteries, a program can stop working
-in Uganda and South Africa, pilot programs have exploded faster than the Ministries of Healths' health strategy and requirements for mobile apps can keep up; they have begun to limit pilot mobile programs to figure this out
Pros:
-increased access to health services for middle- and low-income communities
-cheaper equipment: $8 eye piece for the iPhone can be used to diagnose malaria and TB (see below)
-has been effective for HIV testing among babies in Zambia and Malawi


<-- This is the prototype microscope that Breslauer et al. designed which can be used to detect Malaria and TB.
Breslauer DN, Maamari RN, Switz NA, Lam WA, et al. (2009) Mobile Phone Based Clinical Microscopy for Global Health Applications. PLoS ONE.
These are pictures taken with the microscope above. A and B show two different blood stains for patients who have Malaria. C show sickle cell anemia blood (arrows = sickles). -->
You're probably thinking, "Sounds great. How does this work in my community??" There are several layers to how mobile technologies are applied in Athens, Georgia to improve health. Stay tuned for part II.
Sources:
(1) http://opinionator.blogs.nytimes.com/2013/03/13/the-benefits-of-mobile-health-on-hold/
(2) http://www.plosone.org/article/info%3Adoi%2F10.1371%2Fjournal.pone.0006320
(3) http://onlineathens.com/health/2013-04-09/more-health-care-help-available-video-links
(3) http://onlineathens.com/health/2013-04-09/more-health-care-help-available-video-links
Tuesday, April 2, 2013
Holes in the safety net: policy challenges
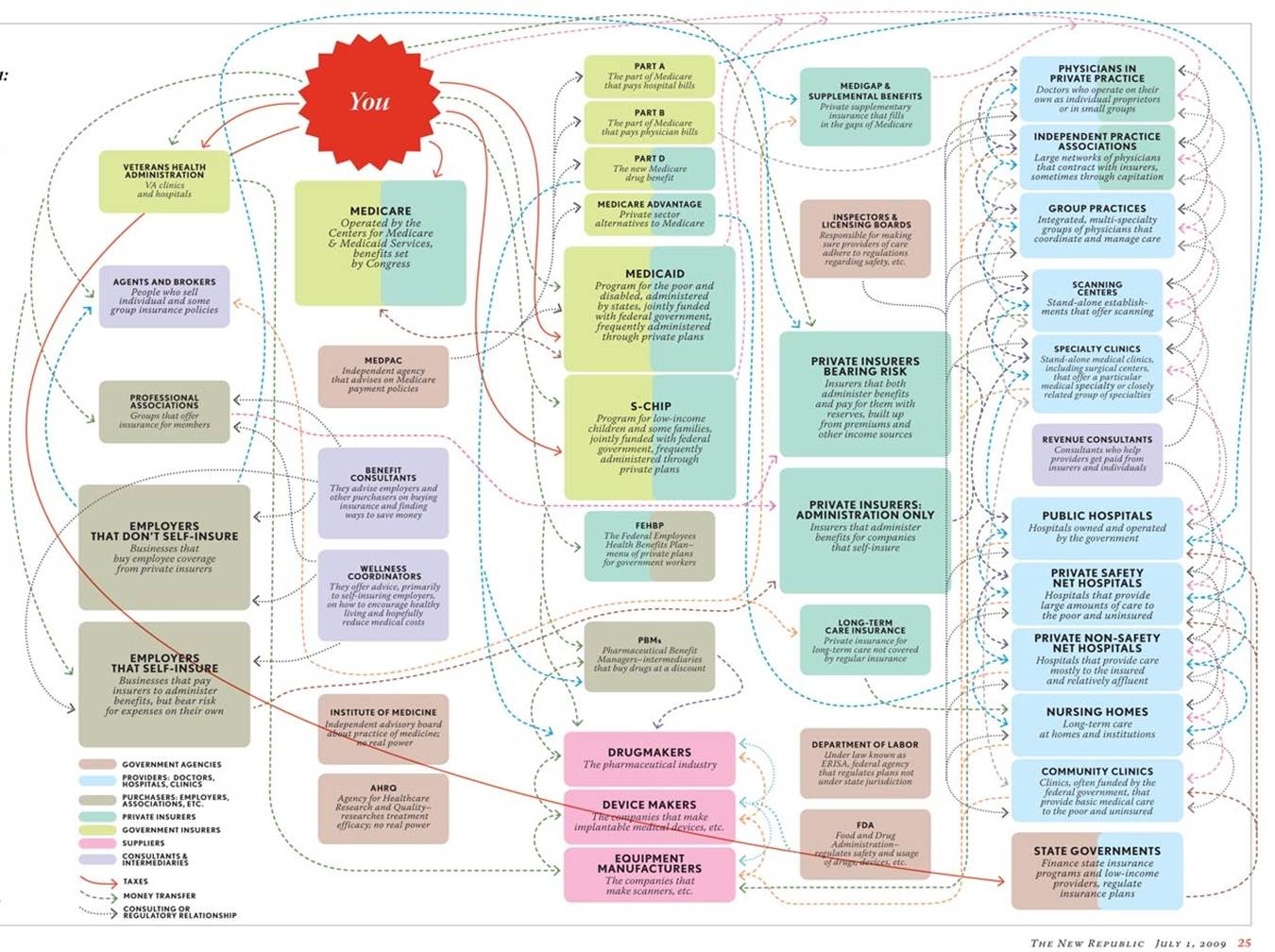
Obviously, there is a significant demand for affordable health care in Athens. So, where can uninsured patients go for care?
The answer is simple (see below and feel free to magnify).

Of course, I am joking. The US health care system is a complicated web of private insurance, safety net providers, emergency rooms, etc. With so many options--or in some cases so few due to barriers--it is no wonder that people have difficulty in navigating the system!
Many underserved patients seek care from a part of the health care system known as the safety net.



The answer is simple (see below and feel free to magnify).
Of course, I am joking. The US health care system is a complicated web of private insurance, safety net providers, emergency rooms, etc. With so many options--or in some cases so few due to barriers--it is no wonder that people have difficulty in navigating the system!
Many underserved patients seek care from a part of the health care system known as the safety net.

The health care safety net refers to health care workers, hospitals, and clinics that offer quality health services to vulnerable populations of patients including those who are uninsured or have Medicaid. Athens is home to a few of these providers. They include the Athens Nurses Clinic, Mercy Health Center, and the Athens Neighborhood Health Center.
Just how adequate is the safety net in addressing patient needs? Let's take a look Athens Neighborhood Health Center (ANHC) and at community health centers in general.
ANHC is our local version of the national community health center (CHC). A CHC is a primary care clinic that provides services to patients regardless of their insurance status or ability to pay. In June 2012, ANHC was promoted to a Federal Qualified Health Center (FQHC). FQHC status means that the center can receive more money from the federal government in order to provide better care to more patients. In general, CHCs provide quality, primary care to patients without regard to the patient's insurance status or ability to pay. In 2010, health centers served over 20 million patients at 8,100 sites.
A few policies are in place to expand the services that CHCs can provide. The Affordable Care Act (aka Obamacare) gives CHCs $11.5 billion over the next 5 years to build new centers and to expand services provided by current ones. In addition, about one-third of CHC patients are covered under Medicaid. Under the ACA, states that choose to expand their Medicaid programs could potentially see an influx of funding to CHCs because more patients will be covered. These policies help CHCs in that they provide additional funding to support their activities; however, they do not address the lack of specialty care in such settings.

Last semester, I researched policy alternatives to increase access to specialty care (neurology, women's clinic, dental services, mental health) in CHCs. From this, I found four possible alternatives:
1. Status quo or "Tin Cup" model--This is based on charity care from local specialists. It is arranged by CHC providers through their informal networks.
2. Medicaid expansion--States that choose to expand Medicaid will, potentially, see an influx of funding to CHCs and can, therefore, use this extra money to increase specialty care provision.
3. Hiring specialists onsite--CHCs can use ACA expansion funds to hire specialists and to buy equipment for onsite use.
4. Collaboration with local public health infrastructure--CHCs can engage in contracts with local hospitals to coordinate speciality and primary care based on existing infrastructure.
After conducting a thorough literature review and evaluation, I concluded that the best-case scenario is for CHCs to collaborate with local hospitals (if available) or to hire onsite specialists (if hospitals are not available).

1. Status quo or "Tin Cup" model--This is based on charity care from local specialists. It is arranged by CHC providers through their informal networks.
2. Medicaid expansion--States that choose to expand Medicaid will, potentially, see an influx of funding to CHCs and can, therefore, use this extra money to increase specialty care provision.
3. Hiring specialists onsite--CHCs can use ACA expansion funds to hire specialists and to buy equipment for onsite use.
4. Collaboration with local public health infrastructure--CHCs can engage in contracts with local hospitals to coordinate speciality and primary care based on existing infrastructure.
After conducting a thorough literature review and evaluation, I concluded that the best-case scenario is for CHCs to collaborate with local hospitals (if available) or to hire onsite specialists (if hospitals are not available).
It is interesting, though, to be an idealistic undergraduate student. I presented this research this past Monday at the 2013 UGA CURO Symposium, and a member of the audience was a physician who had actually tried to collaborate with hospitals to arrange for specialty care in CHCs. It did not go over well. He said that at every level of hospital bureaucracy, he faced red tape and POLITICAL UNFEASIBILITY. None of the hospital administrators wanted to collaborate.
This experience has taught me two things. First, as great as it is to do policy analysis and to find the best of all possible worlds, the reality is we can not implement the best choice. It would be more realistic to work within the constraints, and, in this case, maybe the political feasibility is so insurmountable that Medicaid expansion, though shady, is actually the better alternative. (Heaven forbid it is do nothing status quo..) Second, despite all of the changes that have been made with the ACA, there are still many challenges ahead for social justice in health care.
To be continued...
This experience has taught me two things. First, as great as it is to do policy analysis and to find the best of all possible worlds, the reality is we can not implement the best choice. It would be more realistic to work within the constraints, and, in this case, maybe the political feasibility is so insurmountable that Medicaid expansion, though shady, is actually the better alternative. (Heaven forbid it is do nothing status quo..) Second, despite all of the changes that have been made with the ACA, there are still many challenges ahead for social justice in health care.
To be continued...
Subscribe to:
Comments (Atom)